

Translate this page into:
Spectrum, Prognostic Factors and Outcome of Commonly Missed Cause of Respiratory Distress in Children
*Corresponding author: Saranyadevi Chinnasamy, Department of Pediatrics, Government Dharmapuri Medical College and Hospital, Dharmapuri, Tamil Nadu, India. saranyadevimbbs@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Chinnasamy S, Balasubramanian R, Jayaraman B, Veerachamy N, Poovan P, Karuppannan S. Spectrum, Prognostic Factors and Outcome of Commonly Missed Cause of Respiratory Distress in Children. Ann Child Health. doi: 10.25259/ACH_25_2024
Abstract
Objectives
Foreign body aspiration (FBA) is one of the important causes of respiratory distress, often missed. Early diagnosis and treatment prevent serious complications and improve the outcome. Our objective is to study the clinical profile, prognostic factors, and outcome of FBA in children.
Material and Methods
A prospective study was done from January 2019 to June 2023 in the Department of Paediatrics, Tertiary Care Centre, Tamil Nadu. Children aged 1 month–12 years presented with a history of FBA, and children brought with respiratory distress whose clinical-radiological findings favour FBA were included. Foreign body (FB) in the ear, nose, and gastrointestinal tract was excluded. Children’s age, sex, severity of hypoxia on arrival, duration between aspiration and diagnosis, duration of bronchoscopy procedure, site and nature of FB, pneumonia, and atelectasis in chest X-ray were the factors taken for analysis and outcome.Chi-square test and multiple logistic regression analysis were used for analysis.
Results
Totally 125 children were admitted with features of FBA. 32%, 52%, and 16% were in the age group of <1 year, 1–3 years, and >3 years respectively. 76% of children brought without a history of FBA came with complaints such as respiratory distress, recurrent respiratory tract infection, and wheezing. Decreased air entry on the one side of the chest was seen in 84% of children and chest X-ray showed same-side hyper-inflation in 72% of children. Computed tomography localized the FB in all cases. After a multiple logistic regression analysis, duration between Foreign body aspiration and diagnosis interval [odds ratio (OR) = 6.62, confidence interval (CI) = 1.22–35.8], duration of bronchoscopy procedure (OR = 3.6, CI = 1.65–7.89), pneumonia and atelectasis in chest X-ray (OR = 5.01, CI = 1.69–14.86) were associated with bad outcome.
Conclusion
A child presents with decreased air entry on one side of the chest and same side chest X ray showed hyperinflation, a FBA in the same main bronchus is the strong possibility. Early diagnosis and removal of FB yield excellent outcomes.
Keywords
Airway foreign body
Atelectasis
Bronchoscopy
Hyperinflation
Respiratory distress
INTRODUCTION
Foreign body aspiration (FBA) is one of the important causes of respiratory distress and represents a major cause of morbidity and mortality in children. Diagnosis of this condition demands a high degree of suspicion since physical examination and chest X-ray have low sensitivity.[1] The FBA continues to be a concerning pediatric problem, accounting for thousands of emergency room visits and more than 1000 deaths each year.[2]
It is more frequent in children younger than 3 years of age.[1] There is a high incidence of FBA in toddlers as they use their mouth to explore the surroundings. They are very much interested in eating groundnut, pomegranate, green peas, corn, etc., which are the food materials commonly aspirated. Food materials are most commonly involved, particularly groundnut, although this could change according to regional feeding habits.[3] Radiographical findings are not confirmatory, but the presence of unilateral obstructive emphysema or atelectasis is important.[1]
Children may not disclose a history of choking or inhaling foreign bodies (FBs) because of limited speech, fear, or embarrassment thereby accounting for the low incidence of history of witnessed aspirations.[3]
The entrance of an FB into the airway and the subsequent presence of it, in any part of the bronchial tree is a serious condition for all the age groups. Complete obstruction of the larynx or trachea can lead to death, and prolonged partial obstruction may cause atelectasis, emphysema, bronchiectasis, or occasionally death. Atypical or prolonged respiratory symptoms should alert the physician, and clinical and radiological findings should be carefully evaluated for a possible FBA.[4]
Delay in diagnosis and treatment of FBA should be avoided to prevent complications. Missed or delayed diagnosis of FBA can result in respiratory problems, ranging from life-threatening airway obstruction to recurrent pneumonia, wheezing, and chronic cough. Undiagnosed FBA can mimic other conditions, and the link between choking and subsequent symptoms may not be made by parents or professionals alike.[4]
If the event is noticed on time, the child is taken to the hospital for FB removal by a rigid bronchoscopy. Aspiration of organic FB leads to airway mucosal inflammation and edema in the acute stage. Further, if FB in the airway is missed that leads to the formation of granulation tissue, which later on can lead to symptoms masquerading as bronchial asthma or recurrent/persistent pneumonia. If the event is unnoticed and there are no specific clinical/radiological findings, the patient may be hospitalized for bronchitis, bronchial asthma, or recurrent pneumonia. Delay in diagnosis leads to dangerous consequences for the health and life of the patient, also makes the bronchoscopy procedure difficult, and increases the duration of the procedure while removing the FB.[4]
Our objective is to study the clinical profile, prognostic factors, and outcome of FBA in children at tertiary care center, which is one of the common causes and often missed diagnosis of respiratory distress in children.
MATERIAL AND METHODS
A prospective study was done in the Department of Pediatrics, in a tertiary care center in Tamil Nadu, India, from January 2019 to June 2023. The study was approved by the Institutional Human Ethics Committee. Informed consent was obtained from the parents.
Inclusion criteria
Children presented with a history of FBA and clinical features and investigations suggestive of FBA in the age group of 1 month–12 years were included.
Exclusion criteria
FB in the ear, nose, and gastrointestinal tract was excluded.
Study procedure
Two different study groups of FBA were enrolled in our study. One group of children present with a history of FBA, and another group is elsewhere treated as lower respiratory tract infection/wheeze came with respiratory distress and was diagnosed as FBA in our institution. Age, sex, initial history, clinical presentation, severity of hypoxia on arrival, duration between aspiration and diagnosis interval, radiological findings [X-ray, computed tomography (CT) chest], rigid bronchoscopy findings (site and nature of FB), duration of bronchoscopic procedure, complications, duration of pediatric intensive care unit (PICU) stay, duration of hospital stay, and the outcome of these children were analyzed.
Children presented with clinical features suggestive of FBA were admitted to PICU. Emergency respiratory support was given to correct hypoxia. Then X-ray chest and CT chest were taken to confirm the diagnosis. After the confirmation of FB, with the help of an anesthetist and ear, nose, and throat surgeon, rigid bronchoscopy was done. After removal of FB, the child was shifted to PICU for further care.
After FB removal, the children discharged within 3 days were taken as a good outcome. The children who needed prolonged ventilation for more than 1 day, prolonged PICU stay for more than 5 days, and death were taken as bad outcomes.
Statistical analysis
Data were entered in Microsoft Excel Software and analyzed using the Statistical Package for the Social Sciences Version 16.0. The distribution of different parameters was mentioned as percentages. Prognostic factors were analyzed using the Chi-square test and multiple logistic regression analysis. The odds ratio (OR) and P-value were calculated. P < 0.05 is taken as significant.
RESULTS
During the study period, a total of 125 children were admitted with features of FBA with male preponderance, male: female ratio of 1.2:1. Forty children (32%) were in the age group of <1 year, 65 (52%) children were in the age group of 1–3 years, and 20 (16%) children in the age group of >3 years. Demographic and clinical features are shown in Table 1.
| S. No | Details | Nos. | Percentage |
|---|---|---|---|
| I | Demographic details | ||
| 1 | Male | 68 | 54.4 |
| 2 | Female | 57 | 45.6 |
| 3 | Urban children | 70 | 56 |
| 4 | Rural children | 55 | 44 |
| 5 | Age | ||
| <1 year | 40 | 32 | |
| 1–3 years | 65 | 52 | |
| >3 years | 20 | 16 | |
| II | Clinical features | ||
| 1 | History of aspiration of foreign body | 30 | 24 |
| 2 | No history of aspiration | 95 | 76 |
| 3 | Breathlessness | 120 | 96 |
| 4 | Cough/Cold | 125 | 100 |
| 5 | Vomiting | 105 | 84 |
| 6 | Fever | 42 | 34 |
| 7 | Recurrent respiratory tract infection | 45 | 36 |
| 8 | Hypoxia on arrival | 95 | 76 |
| 9 | Decreased air entry on one side | 105 | 84 |
| 10 | History of intubation on admission | 5 | 4 |
| III | Radiological findings | ||
| 1 | X-ray shows unilateral hyperinflation | 68 | 54.4 |
| 2 | X-ray shows unilateral hyper-inflation with atelectasis | 22 | 17.6 |
| 3 | X-ray shows pneumonia | 12 | 9.6 |
| 4 | X-ray shows pneumonia with atelectasis | 23 | 18.4 |
In our study, the youngest and oldest ages were 3 months and 8 years, respectively. In our study, 56% (70) and 44% (55) of children were brought from urban and rural areas, respectively. Only 24% (30) of the children were brought with a history of aspiration by the parents; the other 76% (95) of children were brought without a history of aspiration, but they came with some other complaints like wheezing, recurrent respiratory tract infection, acute onset of breathlessness, etc. Detailed clinical examination and correlation of radiological investigation helped us to diagnose the FBA in those cases.
All the children (100%) had a history of cold and cough and vomiting in 105 (84%) children, 120 (96%) children had breathlessness, 5 (4%) children presented with severe hypoxia with impending respiratory failure necessitating intubation, 45 (36%) children treated as recurrent respiratory tract infection in various hospitals and diagnosed and treated as FBA in our hospital. Because of late presentation, 42 (34%) children presented with fever due to secondary complications [Table 1].
Thirty children (24%) admitted in the hospital within 24 h of aspiration, whereas 50 (40%) children were admitted in 1–5 days, and 45 (36%) children admitted after 5 days of FB aspiration.
On clinical examination, 84% of children presented with decreased air entry on one side due to FB impacted at the right or left main bronchus, which was a characteristic feature of FBA.
In our study, chest X-ray showed unilateral hyperinflation in 68 children (54.4%), unilateral hyperinflation with atelectasis in 22 (17.6%), pneumonia in12 (9.6%), and pneumonia with atelectasis in 23 (18.4%).
CT chest showed FB as the radiolucent filling defect in all the children, whereas 45.5% of CT showed FB with secondary complications like pneumonia and/or atelectasis. All the children underwent rigid bronchoscopy after obtaining informed consent from parents.
Most of the Foreign bodies in our study was groundnut (42.4%), followed by pomegranate (23.2%), corn (14.4%), and green peas (4.8%) [Table 2]. The most of the Foreign bodies were present in the right main bronchus (64%), followed by the left main bronchus (22.4%), carina (9.6%), and trachea (4%) [Figure 1].
| S. No | Nature of FB | Nos (%) | S. No | Nature of FB | Nos (%) |
|---|---|---|---|---|---|
| 1. | Ground Nut | 53 (42.4) | 9. | Bangle | 1 (0.8) |
| 2. | Pomegranate | 29 (23.2) | 10. | Beetle | 1 (0.8) |
| 3. | Corn | 18 (14.4) | 11. | Sapota Seed piece | 1 (0.8) |
| 4. | Peanut | 6 (4.8) | 12. | Coconut Shell | 1 (0.8) |
| 5. | Chicken Piece | 5 (4) | 13. | Rice | 1 (0.8) |
| 6. | Custard apple seed | 2 (1.6) | 14. | Wooden Piece | 1 (0.8) |
| 7. | Guava piece | 2 (1.6) | 15. | Stone | 1 (0.8) |
| 8. | Coconut Piece | 2 (1.6) | 16. | Beetle Nut | 1 (0.8) |
FB: Foreign body
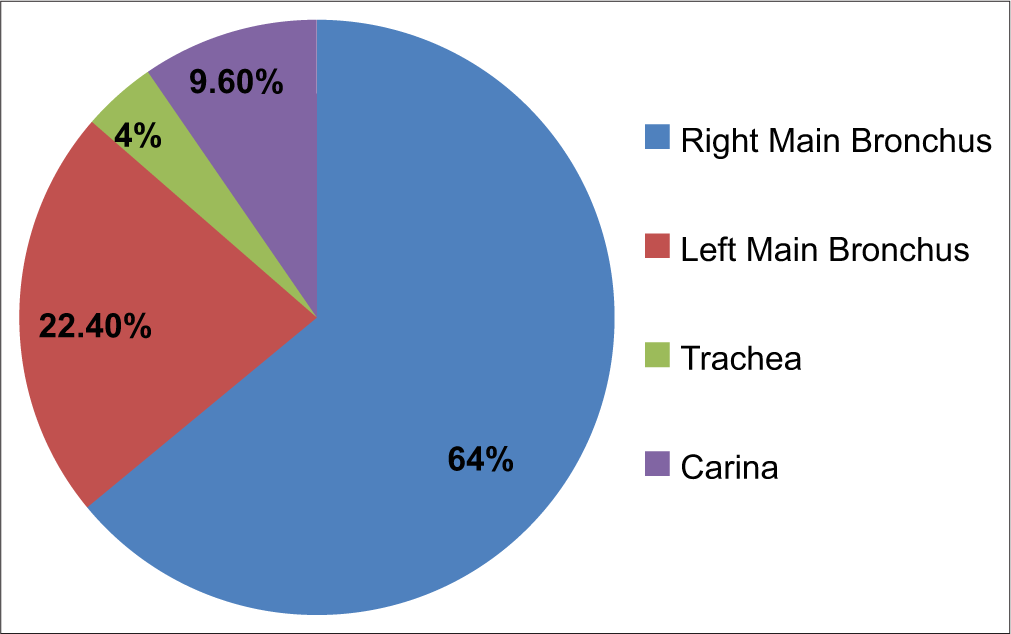
- Location of foreign body in children.
Majority of the children, i.e., 90 (72%), were discharged on day 3 or 4. 32 (25.6%) children needed more than 5 days of PICU stay, and 3 (2.4%) children died due to complications.
Age <1 year (P < 0.01), duration between aspiration and diagnosis interval (>5 days) (P < 0.001), duration of bronchoscopy procedure for removal of FB (P < 0.001), pneumonia and atelectasis in X-ray (P < 0.001), and organic FB (P < 0.004) were associated with bad outcome as per study definition [Table 3].
| S. No | Factors | Chi-square test value | P-value |
|---|---|---|---|
| 1 | Age | 47.18 | P<0.01 |
| 2 | Sex | 2.180 | P<0.14 |
| 3. | Severity of hypoxia on arrival | 0.426 | P<0.514 |
| 4. | Duration between aspiration and diagnosis | 46.3 | P<0.001 |
| 5. | Type of foreign body | 0.165 | P<0.004 |
| 6. | Site of foreign body | 1.673 | P<0.643 |
| 7. | Pneumonia/atelectasis in chest X-ray | 22.5 | P<0.001 |
| 8. | Duration of procedure | 102.3 | P<0.001 |
| Logistic regression analysis | |||
| S. No | Factors | OR | CI |
| 1 | Duration between aspiration and diagnosis interval | 6.62 | 1.22–35.8 |
| 2 | Pneumonia and atelectasis in chest X-ray | 5.01 | 1.69–14.86 |
| 3 | Duration of bronchoscopy procedure | 3.6 | 1.65–7.89 |
OR: Odds ratio, CI: Confidence interval
After multiple logistic regression analysis, interval between aspiration and diagnosis [OR = 6.62, Confidence interval (CI) = 1.22–35.8], duration of bronchoscopy procedure (OR = 3.6, CI = 1.65–7.89), pneumonia and atelectasis in chest X-ray (OR = 5.01, CI = 1.69–14.86) were associated with prolonged PICU stay, more ventilatory support (25.6%), in many children and death in three children [Table 3].
DISCUSSION
FBA is quoted as the fifth cause of non-infectious death among 1–3 years and the primary cause of unintentional death in babies under 12 months. FBA is a very serious common problem in children.[5] Any delay in its diagnosis and management can result in devastating consequences.[6]
The most commonly affected age group was 7 months–14 years in a study by Orji and Akpeh.[3] In our study the minimum age is 3 month,the maximum age is 8 years.
Lima and Fischer mentioned that the parents may unconsciously forget to mention a choking episode during initial contact with the clinician, but he/she can remember it in up to half of the situations when directly questioned about such an event. Hence, it is better to ask about the history of aspiration in any child with sudden onset of breathlessness in <3 Years of age.[1] FBA is common in these age group because of the developmental vulnerability of young child airway and underdeveloped ability to swallow food.[7]
In Orji and Akpeh study, the occurrence of witnessed aspiration was in 47% of children.[3] In our study, only 24% of children are brought with history of aspiration of FB, while 76% of parents did not mention any aspiration history, but they brought the children for some other complaints. Hence, a high index of suspicion is needed when the child presented with respiratory symptoms with decreased breath sound in one side of the chest.
In our study, 24% of children were diagnosed within 24 h, 40% of children diagnosed in 1–5 days, 36% of children diagnosed after 5 days. Delayed diagnosis of FBA (>3 days) was significantly more in younger children as well as in children with no history of witnessed aspiration, negative chest examination, and no radiological sign, as reported by Orji and Akpeh.[3] Delayed diagnosis of FBA significantly associated with prolonged hospital stay, ventilator management, and poor outcome reported in many studies.[5,6]
In our study, 84% of children had unilateral decreased air entry on examination. According to Orji and Akpeh study, 96% of patient had a history of aspiration, and decreased air entry on one side.[3] When the child is brought with acute onset of breathlessness, reduced air entry on one side with same-side hyperinflation in chest X-ray is the pathognomonic finding of FBA.
In our study, chest X-ray showed unilateral hyperinflation in 54.4%, hyperinflation with atelectasis in 17.6% of cases whereas that unilateral hyperinflation in chest X-ray was 39.8% and 40.7% reported by Girardi et al.,[8] and Boufersaoui et al.,[9] respectively. Whenever chest X-ray shows unilateral hyperinflation, it is better to rule out a unilateral obstruction in the main bronchus by FBA, due to the ball-valve effect of FB, unilateral hyperinflation may occur due to the ball-valve effect of FB.[10]
In our study, CT chest localized FB in 100% of children. Pitiot et al., stated that the use of CT chest with multi-planner reconstruction is a reliable alternative to diagnostic bronchoscopy (under general anesthesia) to diagnose the FBA in children especially in asymptomatic patients.[11] A rigid bronchoscopy in children is a high-risk procedure, hence it may be reasonable to carry out a CT chest before rigid bronchoscopy to diagnose the FBA. CT chest is advised when there are no definitive clinical features of FBA and inconclusive chest X-ray findings in highly suspected cases. In our study CT chest was done in 80 children.It helped to detect, identify the site and nature of FB.
The majority of aspirated objects are organic in nature, mainly food materials. In our study, groundnut (42.4%) is the most common FB,[1,3,4,9,12] followed by pomegranate (23.2%), corn (14.4%), and green peas (4.8%).
The high incidence of aspirated seeds is related to the absence of molar teeth development and immature mastication. Therefore, offering chunks of food and seeds of any kind (groundnut, pomegranate, corn, green pea) to this age group should be avoided. It is also strongly recommended that younger children should not be allowed to play with small plastic or metallic objects. Surprisingly, however, plastic toys are not a frequent cause of FBA in developing countries but they represent more than 10% of those identified in the developed world.[4] However, button battery ingestion causes very serious complication and death in children. The different cultural, regional, feeding habits and available food materials present in various parts of the world are the main reasons for various natures of FB aspirated by the children.[4,9]
In Karakoc et al., study, FBs were localized in the right main bronchus in 55.1% of children.[4] In our study, the majority of FB localized in the right main bronchus (64%). The right main bronchus is the site where FBs are most commonly found, likely due to the greater diameter and lesser angle of divergence of the right bronchus in comparison with the left bronchus and therefore, creating a relatively straight pathway from the larynx to bronchus.[13]
According to a study done at Children’s Hospital Medical Center, Cincinnati,[5] younger age, plant seed, longer surgical duration, pneumonia before the procedure, and spontaneous ventilation mode were associated with intraoperative hypoxia. In our study, the interval between aspiration and diagnosis, X-ray showing pneumonia and atelectasis, and duration of bronchoscopic procedure were significantly associated with prolonged hospital stay and ventilatory management.
Due to low functional residual capacity in younger children, they will not tolerate hypoxia during bronchoscopy. Whenever delay in diagnosis, it leads to migration of FB, formation of edema and granulation tissue around the FB, which prolongs the bronchoscopy procedure and difficulty in the removal of FB.[14]
When children are brought with secondary complications, the outcome is poor, and increased risk of mortality, is reported in many studies.[5,15] In the study by Wanstreet et al.,[16] the death rate was 3.7%. Even though many children were brought with a negative history of FBA, a high index of suspicion, earlierdiagnosis, and removal of FB yielded good outcomes in our study (death rate was 2.7%).
“Prevention is better than cure” is the most appropriate statement for FBA in children. Parents should be educated about the possibility of FBA while children eat nuts, seeds, etc., and play with small objects. It is the duty of the pediatrician to educate the parents about the clinical features, complications, and prevention of FBA in younger children.[13,17]
CONCLUSION
FBA is one of the important causes of respiratory distress in children. In most of the situation, parents may not give the history of aspiration. Even though there is no history of aspiration, findings of decreased air entry on one side the chest and same side hyperinflation on Chest X ray strongly suggest FBA. Early diagnosis of FBA leads to safer removal and excellent outcome. The longer duration between FB aspiration and diagnosis interval, complications in chest X-ray, and prolonged bronchoscopy procedures are associated with poor outcomes.
Author contributions
SD: Guarantor of the paper, management of the patients, design and co-ordination of the work, review of literature, analysis and interpretation of data and drafted the first manuscript; RB: Protocol development, supervising the study and critical review; BJ: Review of literature, analysis, and interpretation of data, drafting the manuscript and critical review; NV: Review of literature, analysis and interpretation of data, drafting the manuscript and critical review; PP: Management of patients, analysis and interpretation of data and review of literature; SK: Management of patients, analysis and interpretation of data and review of literature.
Ethical approval
The research/study approved by the Institutional human Ethics Committee, Government medical College Hospital, Dharmapuri, Tamil Nadu, number 44/2023, dated 10th August 2023.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Conflicts of interest
Balaji Jayaraman is on the Editorial Board of the Journal.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
Financial support and sponsorship: Nil.
References
- Foreign Body Aspiration in Children. Paediatr Respir Rev. 2002;3:303-7.
- [CrossRef] [PubMed] [Google Scholar]
- The National Cost Burden of Bronchial Foreign Body Aspiration in Children. Laryngoscope. 2015;125:1221-4.
- [CrossRef] [PubMed] [Google Scholar]
- Tracheobronchial Foreign Body Aspiration In Children: How Reliable are Clinical and Radiological Signs in the Diagnosis? Clin Otolaryngol. 2010;35:479-85.
- [CrossRef] [PubMed] [Google Scholar]
- Late Diagnosis of Foreign Body Aspiration in Children with Chronic Respiratory Symptoms. Int J Pediatr Otorhinolaryngol. 2007;71:241-6.
- [CrossRef] [PubMed] [Google Scholar]
- Foreign Body Aspiration In Children: The Value of Diagnostic Criteria. Int J Pediatr Otorhinolaryngol. 2009;73:963-7.
- [CrossRef] [PubMed] [Google Scholar]
- A New Clinical Algorithm Scoring for Management of Suspected Foreign Body Aspiration in Children. BMC Pulm Med. 2017;17:61.
- [CrossRef] [PubMed] [Google Scholar]
- Two New Radiological Findings to Improve the Diagnosis of Bronchial Foreign-body Aspiration in Children. Pediatr Pulmonol. 2004;38:261-4.
- [CrossRef] [PubMed] [Google Scholar]
- Foreign Body Aspiration in Children: Experience from 2624 Patients. Int J Pediatr Otorhinolaryngol. 2013;77:1683-8.
- [CrossRef] [PubMed] [Google Scholar]
- Foreign body aspiration In: Ghai OP, Paul VK, Aravind B, eds. Ghai Essential Pediatrics (9th ed). New Delhi: CBS Publishers and Distributors; 2019. p. :193. Ch. 15
- [Google Scholar]
- The Use of CT-scan in Foreign Body Aspiration in Children: A 6 Years' Experience. Int J Pediatr Otorhinolaryngol. 2017;102:169-73.
- [CrossRef] [PubMed] [Google Scholar]
- Factors Predicting Early Diagnosis of Foreign Body Aspiration in Children. Pediatr Emerg Care. 2005;21:161-4.
- [Google Scholar]
- The Risk of Foreign Body Aspiration in Children Can Be Reduced with Proper Education of the General Population. Int J Pediatr Otorhinolaryngol. 2007;71:311-5.
- [CrossRef] [PubMed] [Google Scholar]
- Bronchoscopy for Evaluation of Foreign Body Aspiration in Children. J Pediatr Surg. 2003;38:1170-6.
- [CrossRef] [PubMed] [Google Scholar]
- The Complimentary Role of Diagnostic and Therapeutic Endoscopy in Foreign Body Aspiration in Children. Int J Pediatr Otorhinolaryngol. 2011;75:1481-5.
- [CrossRef] [PubMed] [Google Scholar]
- Airway Foreign Bodies in Pediatric Patients: An Analysis of Composition and Age via HCUP KID. Int J Pediatr Otorhinolaryngol. 2021;142:110559.
- [CrossRef] [PubMed] [Google Scholar]
- Complications of Tracheobronchial Foreign Body Aspiration in Children: Report of 5 Cases and Review of the Literature. Rev Hosp Clin Fac Med Sao Paulo. 2002;57:108-11.
- [CrossRef] [PubMed] [Google Scholar]




