

Translate this page into:
Improving Milk Donation at a Comprehensive Lactation Management Center and its Implications on Post-natal and Post-operative Ward Neonates – A Quality Improvement Project
*Corresponding author: Jyoti Kandpal, Department of Pediatrics, Government Dharmapuri Medical College Hospital, Dharmapuri, Tamil Nadu, India. kandpalj1111@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Kandpal J, Balasubramanian R, Veerachamy N, Karuppannan S, Jayaraman B, Poovan P. Improving Milk Donation at a Comprehensive Lactation Management Center and its Implications on Post-natal and Post-operative Ward Neonates – A Quality Improvement Project. Ann Child Health. doi: 10.25259/ACH_26_2024
Abstract
Objectives
To improve monthly milk donation by 30% from 25.4 L to 33 L over 17 months in a comprehensive lactation management center (CLMC) and to study its implications on postnatal and postoperative ward neonates.
Material and Methods
This is a quality improvement (QI) project, conducted from Jan 2022 to May 2024 in three phases: Baseline (Jan-Dec 2022), Intervention (Jan-Dec 2023), and sustenance (Jan-May 2024). A QI team was formed and factors for reduced milk donation were identified. Interventions were planned in two PDSA (Plan Do study Act) cycles to improve awareness among mothers and staff nurses of postnatal (PN)-Postop ward regarding benefits of breastmilk, human milk bank, PDHM, increasing nutrition of mothers and to improve milk collection facilities. The monthly outcome measures were number of donors, average volume of milk collected, volume of milk disbursed, number of beneficiaries, the rate of exclusive breastfeeding, morbidities & mortality in PN-Postoperative ward. Study variables of all three phases were analyzed using QI macros 2020.
Results
The mean (SD) monthly donated milk volume increased from 25.4L (2.5) in baseline to 40.0 L(2.4) and 39.3L (1.03) in intervention and sustenance phase respectively (P < 0.0001). Milk disbursed to PN-Postop ward increased from 6.4L (1.1) in baseline phase to 13.1L(3.8) and 14.5L (0.54) in subsequent phases. Beneficiaries increased from 43(35-49.7) to 68(56.7-77) and 110 (105-120). Exclusive breastfeeding rates improved from 70% to 97% and 99%. Postnatal admissions due to sepsis, feed intolerance, or dehydration decreased from 25.5(23.7-26) to 5(4-6.2) and 5(5-5) after intervention (P < 0.001). Mortality decreased from 0.049% in baseline to 0.016% in intervention phase. However, there were no deaths in sustenance phase (P = 0.011).
Conclusion
QI measures help to motivate more mothers to donate more milk. This improves number of beneficiaries and volume of milk disbursed to neonates in postnatal & postoperative ward which improves their outcomes.
Keywords
Donor human milk
Exclusive breastfeeding
Human milk bank
Postnatal ward babies
Sepsis
INTRODUCTION
Breastfeeding has immense benefits for newborn health.[1-4] Human milk contributes to the developing immune system because it contains antimicrobial, anti-inflammatory, immuno-regulatory agents and living leukocytes.[1] Mothers’ own milk is the best nutrition for a neonate.[5-8] When the mother’s milk is not available, or the mother cannot provide milk, pasteurized donor human milk (PDHM) from a human milk bank (HMB) is the next best possible option for infants.[2] Our sick newborn care unit (SNCU) has an attached comprehensive lactation management center (CLMC)-HMB. The CLMC was established in March 2020, and it screens the donors, collects, processes, stores, and dispenses human milk, which has been voluntary donated by nursing mothers who are not biologically related to the beneficiaries.[9,10] HMBs have supported numerous babies even during COVID time.[11,12]
Exclusive breastfeeding rate in India is only 63.7% (National Family Health Survey-5).[13] In this background, getting donation from mothers is a huge challenge. Based on our CLMC data, the average donation from January to December 2022 was approximately 25.4 L/month. Immediately after delivery, due to pain or unawareness, postnatal and post-cesarean mothers are not able to initiate feed, and hence, relatives or nearby family members give cow’s milk to the baby. Postnatal ward mothers do not get adequate nutrition and guidance regarding exclusive breastfeeding, proper positioning, and attachment to establish lactation. When there is a scarcity of mothers’ milk, apart from lactational counseling, providing PDHM can prevent use of other sources of milk and its complications. Faulty feeding with formula or cow milk predisposes neonatal sepsis, feed intolerance, dehydration in many instances, and even death. That’s why there is an urgent need to improve milk donation (PDHM) from milk banks, which can be given to babies in postnatal and post-operative (PN-Postop) wards when mothers’ milk output is poor.
We can increase the volume of milk collection per month through increasing the number of donors/months by encouraging mothers from the postnatal ward. If this milk is given to postnatal or post-operative ward babies, it will reduce postnatal admissions due to breastfeeding issues, faulty feeding, feed intolerance, sepsis, and dehydration.
QI project is a systematic approach that uses a multi-intervention modality to improve healthcare quality.[14] Hence, our objective is to carry out a QI project to improve milk donation in our CLMC. The objective was to improve milk donation by 30% from 25.4 L/month to 33 L/month over 17 months and to study its implications in PN-Postop ward neonates.
MATERIAL AND METHODS
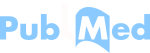
The study is a QI project being carried out at a CLMC attached to an SNCU in a tertiary care center in Tamil Nadu over 29 months, from January 2022 to May 2024. Baseline phase was from January to December 2022, the intervention phase consists of 2 cycles – plan do study act (PDSA) 1 from January to June 2023 and PDSA 2 from July to December 2023, and the sustenance phase was from January to May 2024. A QI team consisting of residents, three staff nurses, and three consultants was formed, and baseline data regarding the number of donors per month, average volume of milk collected per month, volume of milk disbursed, number of beneficiaries per month, the rate of exclusive breastfeeding in PN-Postop ward and data regarding postnatal morbidities (admissions due to sepsis, feed intolerance, and dehydration) and mortality were collected. During the baseline phase, the root cause analysis for reduced milk donation was done, and problems were identified and depicted using a fishbone diagram [Figure 1]. Key drivers and change ideas are identified [Table 1]. There was a lack of adequate counseling for mothers, caregivers, and staff. There was limited availability of lactational counselors and equipment (breast milk pumps). There was a limited donation from PN-Postop wards while demand was more especially for the babies born by cesarean section.
| S. No. | Primary drivers | Secondary drivers | Change ideas |
|---|---|---|---|
| 1. | High demand for PDHM in postnatal wards | Delayed initiation of feeding | Skin to skin care at birth and early rooming in |
| Separation of mother and baby for babies needing observation/admission after birth | Early expression of colostrum and 2–3 hourly milk expression including night expression | ||
| Breastfeeding issues in postnatal ward | One to one counseling for resolving breastfeeding issues | ||
| 2. | Poor awareness about milk donation in mothers | Shortage of lactational counselors in unit – only 1 dedicated staff for counseling | Empower postnatal nurses to support lactation |
| Only verbal counseling at a specific time – some mothers are missed | Use of educational photos, pamphlets and videos for PN-Postop ward | ||
| Limited involvement of postnatal nurses in counseling mothers on breastfeeding and milk donation | Empower postnatal nurses to support lactation | ||
| 3. | Reduced milk donation at CLMC | Poor family support and myths about milk donation | Counseling family members along with mother and addressing doubts and myths by consultants |
| ~ HMB building is away from postnatal ward~Lack of access to milk bank for PN mothers | Establishing milk expression area in PN-postop ward |
CLMC: Comprehensive lactation management center, PN-postop: Postnatal and postoperative, PDHM: Pasteurized donor human milk, HMB: Human milk bank
- Fishbone analysis showing deficit for milk donation. PN: Postnatal
The intervention phase consisted of two PDSA cycles. Each cycle consisted of a set of interventions, which were introduced every 6 months and added to the previous interventions. PDSA cycle 1 consisted of providing early breastfeeding support, daily motivational sessions (mother-to-mother motivation sessions), lactational counseling in HMB by lactational support staff, and consultants for mothers with feeding issues. It also included improving daily postnatal counseling with audiovisual aids and educational materials to resolve breastfeeding issues and improving awareness regarding the benefits of mother milk, PDHM, maternal nutrition, functioning of HMB, and the harms of giving cow’s milk or formula milk.
PDSA cycle 2 consisted of weekly milk bank performance audits, weekly appreciation of mothers donating more milk, maintenance of records of mothers with poor milk output, arranging milk collection center in PN-Postop ward, increasing awareness about exclusive breastfeeding and HMB among PN-Postop ward nurses, and improving maternal nutrition by providing nutrient-rich foods.
The sustenance phase consisted of the maintenance of the above interventions. Data of study variables for intervention and sustenance were collected prospectively. Study variables of all three phases were analyzed using QI macros 2020.
Statistical analysis
Run charts and statistical process control p-charts were used for outcome measures using QI Macros (version 2020). The normality of data was checked with Kolmogorov–Smirnov Z test. Continuous variables were compared by Student’s t-test if data were normally distributed or Mann–Whitney U-test for non-normal distribution. Proportions were compared by the Chi-square test or fisher’s exact test if at least one cell has a frequency <5. Analysis of variance for normal distribution and Kruskal–Wallis test for non-normal data were used for comparison of three groups.
RESULTS
The average milk collection per month in the baseline phase was 25.4 L (2.5) [Mean (Standard deviation)], which increased to 39.7 L (3.2) after PDSA cycle 1 and 40.2 L (1.6) after PDSA 2, which corresponds to 40.0 L (2.4) during the intervention phase and 39.3 L (1.03) during sustenance phase [Figure 2]. This amounts to an increase in milk collection from an average of 0.85 L/day to 1.33 L/day in the intervention phase and 1.31 L/day in sustenance space.

- Statistical process control chart showing volume of milk collected at human milk bank in all three phases. UCL: Upper control line, LCL: Lower control line, PDSA; Plan Do Study Act
Table 2 compares study variables across different phases. There was significant improvement (P = 0.00001) in the volume of milk disbursed to the postnatal post-operative ward from 6.4 L (1.1) in the baseline phase to 13.1 L (3.8) in the intervention phase and 14.5 L (0.54) in sustenance phase. This led to the increase in the total number of beneficiaries in a median, interquartile range 119.5 (99.75–139) in the baseline phase to 164 (154.55–178.75) in the intervention phase 297 (264–300) in the sustenance phase. There was an increase in the number of beneficiaries in the PN-Postop ward from 43 (35–49.75) in the baseline phase to 68 (56.75–77) in the intervention phase and 110 (105–120) in the sustenance phase.
| S. No. | Process Indicators | Baseline phase (B) | Intervention phase (I) | Sustenance phase (S) | P-value |
|---|---|---|---|---|---|
| 1. | *Number of donors/month | 418 (395.5–427.5) | 476.5 (449.25–504.5) | 473 (460–479) | 0.00965a B vs. I: 0.0085 B vs. S: 0.00771 I vs. S: 0.99 |
| 2. | #Average donated milk volume per month (L) | 25.4 (2.5) | 40.0 (2.4) | 39.3 (1.03) | 0.00001a B vs. I :0.00001 B vs. S: 0.0001 I vs. S: 0.97 |
| 3. | *Total number of beneficiaries per month | 119.5 (95.75–139) | 164 (154.55–178.75) | 297 (264–300) | 0.00001a B vs. I: 0.01373 B vs. S: 0.00001 I vs. S: 0.00001 |
| 4. | *Number of beneficiaries per month (in PN-postop ward) | 43 (35–49.75) | 68 (56.75–77) | 110 (105–120) | 0.00001a B vs. I: 0.00056 B vs. S: 0.00001 I vs. S: 0.00001 |
| 5. | #Volume of milk disbursed to PN-postop ward/month (L) | 6.38 (1.1) | 13.1 (3.8) | 14.48 (0.54) | 0.00001a B vs. I: 0.00001 B vs. S: 0.00001 I vs. S: 0.0399 |
| 6. | *No of babies with postnatal morbidities/month | 25.5 (23.75–26) | 5 (4–6.25) | 5 (5–5) | 0.00001b B vs. I: 0.00001c B vs. S: 0.00188c I vs. S: 1c |
| 7. | Deaths (%) (from PN-postop ward)/total babies in postnatal ward | 4/8014=0.049 | 1/6026=0.016 | 0 | 0.011d B vs. I: 0.012f B vs. S: 0.005f I vs. S: 0.042f |
| 8. | Exclusive breastfeeding rates % (PN-postop ward) | 70 | 97 | 99 | <0.001e B vs. I: 0.001 B vs. S: 0.001 I vs. S: 0.23 |
eChi-square test, ftwo-proportion z-test. PN-postop: Postnatal and postoperative. Numbers in bracket indicate -*Median (Interquartile range)
The rate of exclusive breastfeeding improved from 70 % in the baseline phase to 97% in the intervention and 99% in the sustenance phase. There was also a significant reduction in postnatal admissions due to sepsis, feed intolerance, or dehydration from 25.5 (23.75–26) in the baseline phase to 5 (4–6.25) in the intervention phase and 5 (5–5) in sustenance phase (P = 0.0001). There was a reduction in death from 0.049% in the baseline phase to 0.016 % in the intervention phase and no deaths in the sustenance phase (P = 0.011)
The median duration of stay of mothers whose babies were well in the PN-Postop ward was 5 (3–7) days, while the median duration of stay of mothers whose babies got admitted from the post-operative ward due to morbidities such as dehydration, sepsis, or feed intolerance was 9 (7–10) days (P = 0.00068).
DISCUSSION
Human milk is the best milk for a neonate. The rate of exclusive breastfeeding till 6 months is still only 63.7% in India.[13] Lack of guidance, unawareness about breastfeeding, and poor nutrition among mothers are significant barriers to achieving 100% exclusive breastfeeding. This issue is particularly critical in the immediate postnatal period when mothers struggle with insufficient milk output. HMBs provide a safe and reliable source of breast milk for neonates whose mothers are unable to provide milk due to illness, inadequate milk output, or other reasons. The HMB concept was introduced in the 1980s, and the first HMB in India was established in 1989 by Dr. Armida Fernandes at King Edward Memorial (KEM) Hospital in Mumbai. As of 2021, the number of HMBs in India is over 90.[9,11,15]
Our HMB was established in March 2020 as a part of a corporate social responsibility project by Indian Oil Corporation. To ensure the successful functioning of the HMB, motivating mothers and encouraging milk donation are crucial. However, donating milk to the HMB is challenging, especially when mothers struggle with inadequate breast milk for their own babies.
Our QI project is a multi-interventional modality to improve healthcare quality in the HMB. The various problems identified in our study included unawareness and unavailability of good nutrition and myths about nutrition. Many mothers were not given a nutritional diet due to the false belief that mothers’ food affects babies’ digestion. Interventions like awareness regarding good nutrition in PDSA cycle 1 and making the availability of good nutrition available in PDSA cycle 2 were made to increase milk bank donation among mothers of the PN-Postop ward in our study.
We taught the mothers regarding proper positioning and attachment for the establishment of lactation in PDSA 1, which is the standard recommendation. Measures were taken to solve breastfeeding issues like retracted nipples, which were carried out in PDSA cycle 1. Awareness regarding milk bank, PDHM, benefits of mother’s milk, and complications of cow’s milk/formula milk were given to mothers and also to family members and grandparents who take care of mother and baby in the PN-postop ward.
This not only helped to increase exclusive breastfeeding in the PN-Postop ward from 70% to 99% in our study but also improved the donation of mother’s milk.
Due to unawareness, attenders used to give cow’s milk or shop milk, which increased sepsis and other complications such as feed intolerance, dehydration, and even death. Due to this QI project, these morbidities were significantly reduced from 25.5 (23.75–26) per month in the baseline phase to 5 (4–6.35) in the intervention phase and 5 (5–5) per month in the sustenance phase.
In our SNCU, around 300 babies were admitted for various reasons per month. As these babies were sick, they could not be started breastfeeding immediately. Mothers of those babies were not able to initiate breastfeeding in the immediate postnatal period and could not sustain breastfeeding. Hence, they went for secondary lactational failure and could not feed their own babies when they were discharged. Awareness about the donation of milk to milk bank to those mothers improved milk donation through this QI project. Continuous milk donation to HMB enabled them to give milk to their own babies after their babies were stable.
These measures not only solved primary lactational failure but also improved lactation in mothers, which increased the donation of milk to the HMB. This helped to ensure the availability of PDHM to PN-Postop ward babies.
In PDSA cycle 2, a weekly performance audit was done, which helped to reanalyze the project outcomes and, identify the gaps, and take further measures. Mothers donating more milk were honored and greeted every week in the PN-Postop ward. By this weekly activity, donor mothers and their families felt proud among other mothers and attenders who were giving cow’s milk to their own. Furthermore, awareness regarding milk donation in HMB reached a wider audience in the PN-Postop ward, and more mothers came forward to donate milk. Apart from mothers, awareness was also given to family members and PN-Postop ward staff nurses regarding the benefits of PDHM in PDSA cycle 2.
The availability of space for milk donation in the PN-Postop ward made it easier and more comfortable for mothers to donate milk. We also made available more breast pumps for milk donation. These measures increased milk donation and improved the quantity and frequency of milk donation in the PN-postop ward. The use of audiovisual aids helped mothers share their worries and solve doubts.
Many QI studies have been done to improve breastfeeding[16,17] and baby-friendly hospital policies[18-20], and many studies have focused on improving milk donation in HMBs, some of which are QI studies.[10,21-23] In a quality initiative by Sivanandan et al. the average daily voluntary milk donation to HMB increased from 0.83 L/day in the baseline phase to 1.16 and 1.14 L/day in the intervention and post-intervention phases, which are comparable to our study. Multipronged QI intervention effort focusing on exclusive breastfeeding improved voluntary milk donation in HMB bank.[21] Another study by Jain et al. showed that dedicated counseling, constant motivation, scheduled timings for milk donation, along sufficient equipment help in improving milk donation, which is similar to our study, except that our study did not focus on scheduled timings.[22] QI initiatives customized to local settings (training of health care providers, one-to-one counseling, and mother-to-mother support groups) can improve milk donation, which is comparable to our study.[23]
Previous studies have highlighted the use of PDHM in babies in the Neonatal Intensive Care Unit, where the outcome is dependent on many factors, such as the health condition of the baby, treatment details, and the course of the disease.[24] Our study focuses on improving milk donation through QI project and its implications in PN-Postop ward babies. The QI project increased the exclusive breastfeeding rate from 70% to 99%, improved milk donation, and made PDHM available for all needy neonates in PN-Postop ward units where cow or formula milk was given before this QI project. Our study shows that postnatal morbidities significantly decreased after starting the QI project in the unit.
A QI study is a better modality to improve our project, where multiple interventions are needed to bring a noticeable effect. However, the limitation of QI projects lies in their requirement for ongoing educational efforts to sustain long-term effects and prevent relapse to previous practices.
Key message
Sustained counseling and efforts increase milk donation to the HMB (CLMC), reduce lactational failure, resulting in higher exclusive breastfeeding rates and a significant reduction in morbidities such as sepsis, dehydration, and mortality in the PN-Postop ward neonates.
CONCLUSION
Continuous counseling and awareness campaigns for mothers, attenders and staff nurses by utilizing audiovisual aids, have proven effective in increasing milk donation in our facility. In addition, improving mother’s nutrition, honoring donor mothers and providing suitable infrastructure, such as breast pumps and dedicated space for milk donation, have contributed to improved milk donation. As a result, PDHM is now more widely available for needy babies, leading to a significant increase in exclusive breastfeeding rate and a corresponding decrease in morbidities among PN-Postop ward neonates which improve neonatal outcomes.
Author contributions
JK: Guarantor of the paper, management of the patients, design and co-ordination of the work, review of literature, analysis and interpretation of data and drafted the first manuscript; RB: Protocol development and supervising the study; NV: Review of literature, analysis and interpretation of data, drafting the manuscript and critical review; SK: Management of patients, analysis and interpretation of data, review of literature and critical review; BJ: Review of literature, analysis and interpretation of data, drafting the manuscript and critical review; PP: Management of patients, analysis and interpretation of data, review of literature and critical review. All authors approved the final version of the manuscript.
Ethical approval
The research/study approved by the Institutional Ethics Committee at GDMCH, Dharmapuri 36A/2021, dated 1st April 2021.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Conflicts of interest
Balaji Jayaraman is on the Editorial Board of the Journal.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
Financial support and sponsorship: Nil.
References
- Evolution of Immune Functions of the Mammary Gland and Protection of the Infant. Breastfeed Med. 2012;7:132-4.
- [CrossRef] [PubMed] [Google Scholar]
- Donor Human Milk for the High-Risk Infant: Preparation, Safety, and Usage Options in the United States. Pediatrics. 2017;139:e20163440.
- [Google Scholar]
- Benefits of Donor Milk in the Feeding of Preterm Infants. Early Hum Dev. 2013;89(Suppl 2):S3-6.
- [CrossRef] [PubMed] [Google Scholar]
- Human Donor Milk for the Vulnerable Infant: A Canadian Perspective. Int Breastfeed J. 2014;9:4.
- [CrossRef] [PubMed] [Google Scholar]
- Oxford-PATH Human Milk Working Group Call to Action for equitable Access to Human Milk for Vulnerable Infants. Lancet Glob Health. 2019;7:e1484-e1486.
- [CrossRef] [PubMed] [Google Scholar]
- Available from: https://www.who.int/initiatives/every-newborn-action-plan [Last accessed on 2024 Jul 10]
- Section on Breastfeeding Breastfeeding and the Use of Human Milk. Pediatrics. 2012;129:e827-41.
- [CrossRef] [PubMed] [Google Scholar]
- Donor Human Milk for Preterm Infants: Current Evidence and Research Directions. J Pediatr Gastroenterol Nutr. 2013;57:535-42.
- [CrossRef] [PubMed] [Google Scholar]
- National_Guidelines_Lactation_Management_Centres.pdf. Available from: https://nhm.gov.in/images/pdf/programmes/IYCF/National_Guidelines_Lactation_Management_Centres.pdf [Last accessed on 2024 Jul 10]
- [Google Scholar]
- The Profile of Donors to a Human Milk Bank in a Developing Nation. Breastfeed Med. 2020;15:135-9.
- [CrossRef] [PubMed] [Google Scholar]
- Role of Human Milk Banks Amid COVID 19: Perspective From a Milk Bank in India. Int Breastfeed J. 2020;15:104.
- [CrossRef] [PubMed] [Google Scholar]
- Exclusive Breastfeeding Practices and its Determinants in Indian Infants: Findings from the National Family Health Surveys-4 and 5. Int Breastfeed J. 2023;18(1):69.
- [CrossRef] [PubMed] [Google Scholar]
- Why Healthcare Leadership Should Embrace Quality Improvement. BMJ. 2020;368:m872.
- [CrossRef] [PubMed] [Google Scholar]
- Developing Global Guidance on Human Milk Banking. Bull World Health Organ. 2021;99:892-900.
- [CrossRef] [PubMed] [Google Scholar]
- Best Fed Beginnings: A Nationwide Quality Improvement Initiative to Increase Breastfeeding. Pediatrics. 2017;140:e20163121.
- [CrossRef] [PubMed] [Google Scholar]
- A Quality Improvement Initiative: Improving First-hour Breastfeeding Initiation Rate among Healthy Newborns. Pediatr Qual Saf. 2021;6:e433.
- [CrossRef] [PubMed] [Google Scholar]
- A Breastfeeding Quality Improvement Project in Rural Primary Care. J Hum Lact. 2016;32:633-41.
- [CrossRef] [PubMed] [Google Scholar]
- Impact of Mother-Baby Friendly Initiative Plus Approach on Improving Human Milk Feeding for Neonates in Hospital: A Quality Improvement Before-and-After Uncontrolled Study. Eur J Pediatr. 2022;181:107-16.
- [CrossRef] [PubMed] [Google Scholar]
- Baby-Friendly as a Regional Collaborative Quality Improvement Project in an Academic Medical Center Environment. J Perinat Neonatal Nurs. 2018;32:136-43.
- [CrossRef] [PubMed] [Google Scholar]
- A Quality Improvement Project to Improve Voluntary Milk Donation in a Human Milk Bank in South India. Med J Armed Forces India. 2023;79:565-71.
- [CrossRef] [PubMed] [Google Scholar]
- Quality Improvement Initiative for a Sustained Increase in Human Milk Donation During the Hospital Stay. BMJ Open Qual. 2023;12(Suppl 3):e002133.
- [CrossRef] [PubMed] [Google Scholar]
- A Quality Improvement Initiative to Increase the Milk Donation to the Human Milk Bank Post-Coronavirus Disease-19 Pandemic. Breastfeeding Medicine. Available from: https://www.liebertpub.com/doi/abs/10.1089/bfm.2023.0124?download=true&journalCode=bfm [Last accessed on 2024 Jul 18]
- [Google Scholar]
- Impact of Human Milk Banking on Neonatal Mortality, Necrotizing Enterocolitis, and Exclusive Breastfeeding-Experience From a Tertiary Care Teaching Hospital, South India. J Matern Fetal Neonatal Med. 2019;32:902-5.
- [CrossRef] [PubMed] [Google Scholar]




