

Translate this page into:
Does Gastric Lavage with Expressed Breastmilk Reduce the Incidence of Necrotizing Enterocolitis among Very-Low-Birth Weight Infants? – A Randomized Controlled Trial
*Corresponding author: B. Adhisivam, Department of Neonatology, Jawaharlal Institute of Postgraduate Medical Education and Research, Puducherry, India. adhisivam1975@yahoo.co.uk
-
Received: ,
Accepted: ,
How to cite this article: Das G, Murugesan A, Gupta S, Adhisivam B. Does Gastric Lavage with Expressed Breastmilk Reduce the Incidence of Necrotizing Enterocolitis among Very Low-Birth-Weight Infants? – A Randomized Controlled Trial. Ann Child Health. doi: 10.25259/ACH_17_2024
Abstract
Objectives:
The objectives of this study were to evaluate whether gastric lavage with expressed breastmilk (EBM) decreases the incidence of necrotizing enterocolitis (NEC) among very low-birth-weight (VLBW) infants compared to standard care.
Material and Methods:
This open-label randomized controlled trial included VLBW infants who were randomized to receive either gastric lavage with EBM (intervention group) or standard care (control group). The primary outcome assessed was the incidence of NEC. Secondary outcomes were mortality, duration of hospital stay, days to achieve full feeds, and weight gain at discharge.
Results:
A total of 99 neonates were enrolled (51 in the intervention group and 48 in the control group). NEC rates were similar in both groups (5.9% vs. 4.2%; P = 0.39). However, there was a significant reduction in mortality in the intervention group (1.9% vs. 14.6%, P = 0.04).
Conclusion:
Gastric lavage with EBM did not reduce the incidence of NEC in the population studied, but there was a significant reduction in mortality in the intervention group.
Keywords
Gastric lavage
Necrotizing enterocolitis
Newborn
INTRODUCTION
Necrotizing enterocolitis (NEC) is a disease of the preterm gut that occurs due to immune dysregulation, inflammation, and intestinal dysbiosis. There are several strategies aimed at reducing the risk of NEC, including antenatal corticosteroids, delayed cord clamping, feeding of the mother’s milk (MOM) to the baby, standardized feeding protocols, and probiotics.[1-4] A few studies have shown reduced incidence of feed intolerance and time to full feeds when gastric lavage was done with expressed breastmilk (EBM).[5] However, there are still concerns regarding NEC association with early feed initiation, especially in those infants with Doppler abnormalities detected antenatally. Very low-birth-weight (VLBW) babies (birth weight <1500 g) are usually kept nil oral after birth for fear of NEC. However, breast milk contains numerous protective bioagents that can prevent NEC. An initial gastric lavage with EBM is a cautious balance between nil oral and minimal enteral nutrition. This procedure can prevent NEC, facilitate early initiation of feeds, and provide bioactive and growth factors, which can improve weight gain and, hence, early discharge. Hence, this randomized controlled trial (RCT) was done to evaluate whether gastric lavage with EBM decreases the incidence of NEC among VLBW infants compared to standard care.
MATERIAL AND METHODS
This open-label randomized controlled trial was conducted in a level III neonatal intensive care unit (NICU) of a tertiary care hospital in Puducherry after due approval from the Institute Ethics Committee. The study was also registered with the Clinical Trials Registry India (CTRI) prospectively (CTRI/2016/11/007507). Preterm VLBW neonates were enrolled after written informed consent from parents. Those infants with evidence of asphyxia, sepsis, and major congenital anomalies were excluded from the study. The enrolled neonates were randomized using computer-generated sequences to receive either gastric lavage with EBM (intervention group) or standard care (control group). Gastric lavage was done using 3–5 mL of MOM under sterile precautions. The first lavage was done within 4 h of delivery and continued 3 h for the 1st 48 h. After a contact period of 15 minutes, the extra residues (if any) were aspirated. Feeds were advanced as per standard NICU protocol.[6] Full feeds were considered to be achieved when feeds of 150 mL/Kg/d were tolerated. Parenteral nutrition was stopped when 120 mL/Kg/d enteral feeding volume was achieved. Neonates were monitored for clinical features of NEC and sepsis, including vomiting, abdominal distention, abdominal wall erythema, tenderness, and bleeding manifestations. NEC was classified according to modified Bell’s staging.[7] Serum calprotectin levels (biomarker for NEC) were done on day 3 and day 7 for all neonates. The neonates in the control group were kept nil oral initially. Apart from gastric lavage with MOM for the intervention group, management was the same in both groups. Baseline neonatal and maternal demographic parameters and risk factors for NEC were collected. Other data, including the use of respiratory support, surfactant administration, presence of patent ductus arteriosus, shock, and sepsis, were collected for both groups. All neonates were followed up for 28 days or discharged, whichever was earlier. The primary outcome evaluated was the incidence of NEC during the study period. The sample size was calculated for a non-inferiority trial using an online calculator “sealed envelope.” With an assumption of reduction of NEC by 10% by the intervention compared to standard care, 67 infants per group were needed for a non-inferiority limit of 5%, a type I error of 0.05, and a power of 0.90. Data on categorical variables were presented as frequencies and percentages. The NEC rates in both groups were compared using the Chi-square test. P < 0.05 was considered significant.
RESULTS
A total of 638 VLBW neonates were assessed for eligibility, and after exclusions, 99 were enrolled (51 in the study group and 48 in the control group) [Figure 1]. The baseline maternal and neonatal characteristics between the two groups were comparable, and their morbidity profile was also similar [Table 1]. The primary outcome NEC was similar in both groups (5.9% vs. 4.2%; P = 1.00). There was a significantly reduced mortality in the intervention group (1.9% vs. 14.6%, P = 0.04, odds ratio [OR]: 0.12 [0.01–0.99]). Other outcomes, such as sepsis, duration of hospital stay, days to full feeds, and weight gain, were similar in both groups [Table 2].
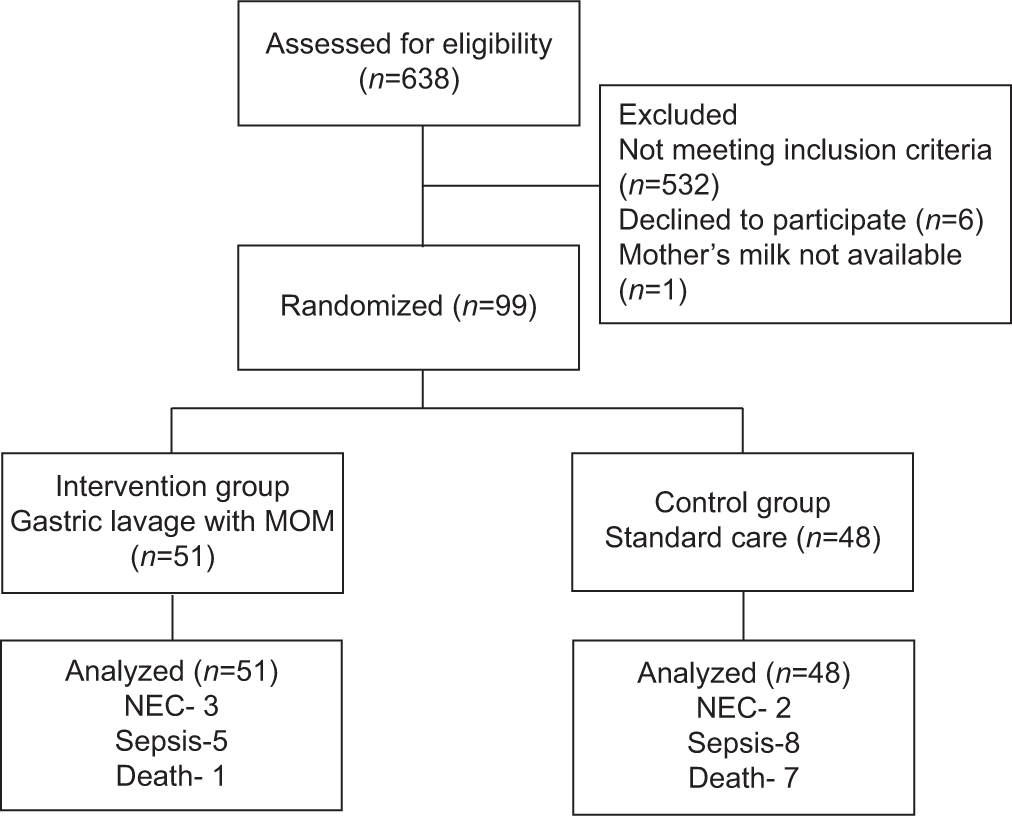
- Consolidated Standards of Reporting Trials flow diagram (CONSORT) flow diagram.
| Parameters | Gastric lavage (n=51) | No lavage (n=48) |
|---|---|---|
| Gestational age in weeks median (IQR) | 30 (28–32) | 31 (29–33) |
| Birth weight in g mean (SD) | 1230 (205) | 1236 (252) |
| Small for gestational age (%) | 25 (49.0) | 28 (58.3) |
| Absent end-diastolic flow (%) | 10 (19.6) | 9 (18.8) |
| Reversal of end-diastolic flow (%) | 1 (1.9) | 1 (2.1) |
| Mode of delivery | ||
| Lower-segment cesarean section (%) | 32 (62.7) | 30 (62.5) |
| Respiratory support (%) | ||
| Mechanical ventilation | 16 (31.3) | 14 (29.2) |
| Surfactant replacement therapy | 13 (25.5) | 10 (20.8) |
| Non-invasive ventilation | 34 (66.6) | 28 (58.3) |
| Patent ductus arteriosus requiring treatment (%) | 9 (17.6) | 12 (25) |
| Asphyxia (%) | 8 (15.7) | 4 (8.3) |
| Shock (%) | 9 (17.6) | 8 (16.7) |
| Caffeine citrate requirement (%) | 38 (74.5) | 23 (47.9) |
| Umbilical vein catheterization (%) | 17 (33.3) | 17 (35.4) |
| Maternal parameters | ||
| Age in years (IQR) | 27 (21–34) | 25 (20–32) |
| Pregnancy-induced hypertension (%) | 27 (52.9) | 27 (56.3) |
| Gestational diabetes mellitus (%) | 12 (23.5) | 5 (10.4) |
| Chorioamnionitis (%) | 0 | 0 |
| Premature rupture of membranes (%) | 12 (23.5) | 9 (18.8) |
| Hypothyroidism (%) | 4 (7.8) | 3 (6.3) |
| Urinary tract infection (%) | 2 (3.9) | 5 (10.4) |
| Antenatal steroid coverage (%) | ||
| Nil | 24 (47) | 25 (52.1) |
| Partial | 20 (39.2) | 17 (35.4) |
| Complete | 7 (13.7) | 6 (12.5) |
IQR: Interquartile range, SD: Standard deviation
| Outcomes | Gastric lavage (n=51) | No lavage (n=48) | P-value |
|---|---|---|---|
| Death | 1 (1.9%) | 7 (14.6%) | 0.03 |
| OR 0.12 (0.01–0.99) | |||
| Culture proven sepsis | 5 (9.8%) | 8 (16.7%) | 0.38 |
| Early-onset sepsis | 5 | 6 | |
| Late-onset sepsis | 0 | 2 | |
| NEC (any stage) | 3 (5.9%) | 2 (4.2%) | 0.39 |
| Stage 1 | 1 | 1 | |
| Stage 2 | 0 | 1 | |
| Stage 3 | 2 | 0 | |
| Day to attain full feeds | 7 (2) | 7 (2) | 0.19 |
| Median (IQR) | Range: 5–19 | Range: 5–16 | |
| Weight at discharge g mean (SD) | 1569 (326) | 1567 (311) | 0.97 |
| Serum calprotectin on day 3 | 202.6+189.2 | 145.7+159.17 | 0.11 |
| Serum calprotectin on day 7 | 184+188 | 135+147.9 | 0.15 |
| Serum calprotectin positive on day 3 | 19 | 11 | 0.13 |
| Serum calprotectin positive on day 7 | 15 | 9 | 0.25 |
IQR: Interquartile range, SD: Standard deviation, NEC: Necrotizing enterocolitis, OR: Odds ratio
DISCUSSION
NEC in neonates is associated with significant mortality and morbidity; hence, preventive strategies are of paramount importance.[1-4] NEC in low- and middle-income countries (LMICs) differs from those seen in the west due to the fact that the majority of the affected infants are much older and the prevalence of fetal growth restriction is high.[8] Low-cost interventions such as antenatal steroids, delayed cord clamping, feeding MOM to the baby, and protocolized feeding are effective in preventing NEC. The use of probiotics has also been shown to reduce the incidence of NEC[3] but cost and storage are a major impediment in resource-limited settings. Gastric lavage with mother’s milk and its effect on feed intolerance has been studied previously in preterm infants and term infants, but there is a lack of data related to gastric lavage and the incidence of NEC among VLBW infants [5,9,10]
About half the study population was small for gestational age (SGA), who are at higher risk for mortality and morbidities, including NEC. The higher prevalence of SGA might be explained by the fact that ours were a referral institute for high-risk pregnancies. Around 20% of these infants had Doppler abnormalities, similar to data from other studies.[11] Antenatal steroid coverage was around 50%, which probably reflects the short duration from admission to delivery. About 63% of the neonates required respiratory support, which mirrors the prevalence of respiratory distress syndrome in this group.[12]
Breastmilk lavage has been previously studied in preterm infants[5], but the enrolled population in the present study was more premature and sicker than those in the previous studies. Moreover, the mean duration to reach full feeds was also much shorter in our study. The median age of attainment of full feeds was similar in both groups (7 days). Weight gain at discharge was also similar in both groups. The incidence of NEC was similar in both groups (5.9% in the study group vs. 4.2% in the control group; P = 0.39). Due to a low event rate of NEC in both groups combined (5.1%; 5/99), we were not able to find any meaningful difference in the rates of NEC. The incidence of NEC has been reported to vary between 7 and 10% in VLBW infants across the world.[8,13] The low incidence of NEC in our study may be due to protocolized feeding, use of only human milk in NICU, and a higher median gestational age of enrolled neonates (only 8% of the enrolled neonates were <28 weeks of gestation).
Calprotectin has been studied as a marker for bowel inflammation and NEC in preterm infants. A calprotectin level of 226 ug/g was taken as the cutoff for positivity based on previous literature.[14] We did not find a significant difference in the proportion of infants who had positive calprotectin levels in both groups. Even among the three infants who had significant NEC (stage 2b or more), calprotectin done on day 7 was normal. One possible explanation is that the levels were done on day 3 and day 7 and not when NEC was diagnosed, leading to the detection of normal levels in these neonates.
Among other secondary outcomes, mortality was significantly lower in the intervention group (1.9% vs. 14.6%, OR: 0.12 [95% confidence interval: 0.01–0.99] P = 0.04). Although the study was not powered to detect any difference in mortality, the difference was statistically significant. It is possible that the difference in mortality was due to a higher sepsis-related mortality in the control group compared to the intervention group. Gastric lavage with MOM has the potential to reduce bacterial adhesion and proliferation in the immature gut, which might have led to this effect.[5]
Early enteral feeding has the benefits of reduced incidence of sepsis and total parenteral nutrition-related complications without any increase in the incidence of feed intolerance or NEC, even in neonates with Doppler abnormalities.[15] Earlier studies evaluated the effects of evacuation of meconium on feed tolerance in preterm infants on the basis that delayed meconium passage might delay feed tolerance and also predispose to infection due to intestinal stasis[10] but failed to show any beneficial results. Anti-infective factors of breast milk are well known to promote colonization of favorable microbes while reducing inflammation. Hence, we assessed the combined effects of early enteral feeding and lavage with MOM in our cohort of VLBW infants. Although NEC rates were similar, lower mortality in the study group suggests early enteral feeding combined with gastric lavage is well tolerated and might be beneficial, even in a cohort with a higher prevalence of SGA and Doppler abnormalities.
There are a few limitations to this study. The desired sample size could not be reached due to changes in feeding protocol in the unit toward a more aggressive enteral feeding regimen; there were lesser infants <28 weeks of gestation (only 8%). Extreme preterm infants are more at risk of feed intolerance and NEC and might have benefited from the intervention. An ongoing large RCT enrolling extreme preterm infants evaluating the effect of intestinal lavage, although with saline, on feed tolerance is currently underway[16] and may be expected to contribute to the evidence in extreme preterm infants.
CONCLUSION
Gastric lavage with MOM is well tolerated without any difference in NEC but with a significant reduction in mortality in preterm VLBW neonates. Regardless of the intervention, early enteral feeding and protocolized hiking of feeds are key to preventing NEC in preterm neonates.
Author contributions
GD and SG: Collected data;
MA: Data analyzed and drafted the manuscript;
AB: Study designed, supervised clinical work, and edited the manuscript
Ethical approval
The research/study approved by the Institutional Review Board at JIPMER, number JIP/IEC/2016/24/818, dated 31th March 2016.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
Financial support and sponsorship
Nil.
References
- An Overview of Systematic Reviews of Randomized-Controlled Trials for Preventing Necrotizing Enterocolitis in Preterm Infants. Neonatology. 2020;117:46-56.
- [CrossRef] [PubMed] [Google Scholar]
- Necrotizing Enterocolitis and Human Milk Feeding: A Systematic Review. Clin Perinatol. 2017;44:49-67.
- [CrossRef] [PubMed] [Google Scholar]
- Probiotics for Preventing Necrotizing Enterocolitis in Preterm Infants: A Network Meta-Analysis. Nutrients. 2021;13:192.
- [CrossRef] [PubMed] [Google Scholar]
- Risk Factors for Necrotizing Enterocolitis: A Prospective Multicenter Case-Control Study. Neonatology. 2018;114:277-84.
- [CrossRef] [PubMed] [Google Scholar]
- Efficacy of Breast Milk Gastric Lavage in Preterm Neonates. Indian Pediatr. 2007;44:199-203.
- [Google Scholar]
- Necrotizing Enterocolitis: Treatment Based on Staging Criteria. Pediatr Clin North Am. 1986;33:179-201.
- [CrossRef] [PubMed] [Google Scholar]
- Risk Factors and Outcome in Neonatal Necrotisingenterocolitis. Indian J Pediatr. 2014;81:425-8.
- [CrossRef] [PubMed] [Google Scholar]
- Meconium Evacuation for Facilitating Feed Tolerance in Preterm Neonates: A Systematic Review and Meta-Analysis. Neonatology. 2016;110:55-65.
- [CrossRef] [PubMed] [Google Scholar]
- Induction of Early Meconium Evacuation Promotes Feeding Tolerance in Very Low Birth Weight Infants. Neonatology. 2007;92:67-72.
- [CrossRef] [PubMed] [Google Scholar]
- Prevalence of Small-for-Gestational-Age and Its Mortality Risk Varies by Choice of Birth-Weight-for-Gestation Reference Population. PLoS One. 2014;9:e92074.
- [CrossRef] [PubMed] [Google Scholar]
- Respiratory Distress Syndrome in VLBW Infants: Changes in Management and Outcomes Observed by the NICHD Neonatal Research Network. Semin Perinatol. 2003;27:288-92.
- [CrossRef] [PubMed] [Google Scholar]
- Global Incidence of Necrotizing Enterocolitis: A Systematic Review and Meta-analysis. BMC Pediatr. 2020;20:344.
- [CrossRef] [PubMed] [Google Scholar]
- Can Fecal Calprotectin Serve as a Screen for Necrotizing Enterocolitis in Infants? Clin Biochem. 2020;84:51-4.
- [CrossRef] [PubMed] [Google Scholar]
- ADEPT-Abnormal Doppler Enteral Prescription Trial. BMC Pediatr. 2009;9:63.
- [CrossRef] [PubMed] [Google Scholar]
- Intestinal Lavage to Promote Enteral Feeding and Prevent Necrotizing Enterocolitis in Extremely Preterm Infants. 2018-2026. Available from: https://clinicaltrials.gov/ct2/show/NCT03631979 [Last accessed on 2024 Jul 15]
- [Google Scholar]




