

Translate this page into:
Cardiac Manifestations in Multi-System Inflammatory Syndrome in Children Temporally Associated with SARS-CoV-2 Infection
*Corresponding author: Muruganantham Balagurunathan, Associate Professor, Department of Pediatrics, PSG Institute of Medical Sciences and Research, Coimbatore, Tamil Nadu, India. murugambbs@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Preethi NS, Balagurunathan M, Palanisamy V, Arumugam J, Doraiswamy V. Cardiac Manifestations in Multi-System Inflammatory Syndrome in Children Temporally Associated with SARS-CoV-2 Infection. Ann Child Health. 2024;1:25-31. doi: 10.25259/ ACH_4_2024
Abstract
Objectives:
The objective of this study was to assess the cardiac manifestations due to MIS-C by echocardiogram and to analyze the outcome and follow-up changes at 2 weeks and 6 weeks.
Material and Methods:
This prospective descriptive study was conducted in a tertiary care center in Coimbatore, Tamil Nadu, for 1 year. The study population included patients diagnosed with MIS-C. Cardiac manifestations were assessed clinically by echocardiogram findings, z-score calculation, and cardiac biochemical markers which were collected during hospital stay and at subsequent review and analyzed.
Results:
A total of 34 MIS-C patients were included in this study, with a median age of 6.5 years. Among the 15 patients with electrocardiogram (ECG) data, 8 (53%) had abnormal ECG findings. Most common findings are sinus tachycardia, sinus bradycardia, and non-specific T wave changes. An abnormal echocardiogram was noted in 27 out of 34 children. Coronary abnormalities were noted in 12 patients, of which seven had coronary dilation, and seven had a coronary aneurysm. Follow-up data were available for 20 patients. Two weeks after discharge, one patient had a persistent coronary aneurysm that resolved at 6 weeks follow-up. All other abnormalities were resolved at 2 weeks follow-up.
Conclusion:
Cardiac involvement is common in MIS-C, as 27 out of 34 children have manifested the same in our study population. These patients with appropriate early management had an excellent short-term outcome with complete resolution of echocardiogram findings.
Keywords
Cardiovascular manifestations
COVID-19
Echocardiogram
Multi-system inflammatory syndrome in children
INTRODUCTION
COVID-19, caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), has led to over 6 million fatalities worldwide[1] and was officially classified as a pandemic on March 11, 2020, by the World Health Organization (WHO).[2] Predominant symptoms included fever, cough, fatigue, and dyspnea, with less frequently reported gastrointestinal manifestations such as diarrhea. The elderly population, aged 65 years or older, faced an elevated risk of developing severe SARS-CoV-2 infection due to a higher prevalence of established comorbidities.[3] While younger adults were also hospitalized for severe illness, the occurrence was significantly lower.[4] Compared to infected adults, most infected children exhibited a less severe clinical course and presented with milder symptoms.[5,6] Asymptomatic infections were also observed with inconsiderable frequency.[5] However, reports emerged from COVID-19 epicenters across Europe documenting clusters of pediatric hospitalizations associated with a severe Kawasaki-like disease and hyperinflammatory shock syndrome.[7,8] The clinical symptoms included pyrexia (>38.5°C) and asthenia. Prevalent gastrointestinal manifestations were abdominal pain, vomiting, and diarrhea. All individuals exhibited a pronounced inflammatory condition, as indicated by elevated levels of C-reactive protein (CRP) and D-dimer. This syndrome was characterized by a temporal correlation with a recent SARS-CoV-2 infection, evidenced by a history of close contact and positive serology.[9] The predominant cardiac involvement ranged from mild-to-severe reduced left ventricular (LV) ejection, arrhythmias, pericardial effusion, coronary artery dilatations, or aneurysms to cardiogenic shock.[10] This emerging syndrome was categorized as “Multisystem inflammatory syndrome in children (MIS-C)” by the US Centers for Disease Control and Prevention (CDC)[11] and WHO[12] and as “Pediatric multisystem inflammatory syndrome temporally associated with COVID-19” by the Royal College of Pediatrics and Child Health.[13] The most frequent therapies for MIS-C include immunoglobulins, vasoactive agents, and corticosteroids.[14] In the present study, we delineate the cardiovascular and clinical manifestations, laboratory findings, and cardiac imaging results of MIS-C observed at our center during a 1-year time frame. The aim of the present study was to assess the cardiac manifestations (by echocardiogram) and laboratory markers due to MIS-C and to analyze the outcome and follow-up changes at 2 weeks and 6 weeks.
MATERIAL AND METHODS
The present study was a descriptive study and was conducted at the Department of Pediatrics, PSG Institute of Medical Science and Research, Coimbatore, for a period of 1 year. The study was initiated after obtaining approval from the Institutional Human Ethics Committee, Ref: PSG/IHEC/2020/Appr/Exp/285, dated December 18, 2020.
The study population included patients diagnosed with MIS-C. As per the CDC, MIS-C was defined as any person below 21 years presenting with fever >38.0°C for more than 24 h, inflammation, severe illness requiring hospitalization, involvement of more than 2 organs after ruling out other differential diagnoses, and positive for SARS-CoV-2 or has recently been in contact with a suspected or confirmed COVID-19 case.[14]
Children with known congenital or acquired cardiac diseases and who were already on cardiotoxic medications such as chemotherapy and immunomodulators were excluded from the study.
A convenient sampling method was used for the study. Considering an absolute error of 5% and a death rate of 1.7% from previous studies,[15] the present study included 34 patients with MIS-C diagnosed during the study period. The formula for sample size calculation for an unknown population was used as follows-
Sample size = Z2 × p(1-p)/e2
The names of the patients were masked in the study, and each patient was allocated a case number. The cardiac status, including heart rate, blood pressure, cardiovascular system findings, perfusion status, and signs of pericardial/pleural effusion at the time of presentation, were clinically assessed and noted. Biochemical markers such as D-dimer, creatine phosphokinase (CPK), CPK-MB, Troponin T, and N-terminal pro-brain natriuretic peptide (NT-Pro BNP) values were also noted. A standard 12 lead electrocardiogram (ECG) was used, and findings such as normal sinus rhythm, sinus tachycardia, arrhythmias, heart block, or any other abnormal findings suggestive of myocarditis or pericarditis were noted. The cardiac status of the children was assessed clinically, and normalization of previously elevated biochemical markers was confirmed during the follow-up.
Echocardiography assessment
All patients suspected of having MIS-C based on the above criteria were subjected to echocardiographic examination as a part of MIS-C evaluation and treatment. LV ejection fraction (LVEF) was evaluated using Simpson’s biplane method; graded as mild with LVEF 41–52%, moderate with LVEF 30–40%, and severe if <30%.[16] The presence/absence of valvular regurgitations (mitral and tricuspid valves) and pericardial effusion were noted. Coronary artery abnormalities were evaluated according to standard guidelines. Coronary artery z-scores were calculated based on the Boston z-score system; the status was graded as dilatation, “z-score 2–2.5;” small aneurysm, “z-score 2.5–5;” medium aneurysm, “z-score 5–10;” and giant aneurysm, “z-score >10,” or internal measurement >8 mm based on the American Heart Association statement paper of the Kawasaki Disease committee.[17]
Detailed echocardiographic examinations were carried out (before starting immunoglobulin or steroids) on admission, mostly done within the first 48 hours of admission and on the day of discharge. Routine follow-ups were planned at 2 weeks and 6 weeks.
All the collected data were compiled in the Microsoft excel sheet. Percentage analysis was done using the Statistical Package for the Social Sciences (SPSS) software version 26. Categorical variables were expressed as percentages, and continuous variables were expressed as mean with standard deviation or median with interquartile range (IQR). The association between categorical variables was analyzed using the Chi-square test. IBM SPSS Statistics ver. 26.0 (IBM Co., Armonk, NY, USA) was used to perform univariate analysis, and P < 0.05 was considered significant.
RESULTS
A total of 34 MIS-C patients were included in this study. The median age of the population was 6.5 years, with IQR 3–10. Among the study subjects, 23 (67.6%) were male. The baseline characteristics of the study subjects, along with the abnormal cardiovascular findings, are presented in Table 1.
| Median age (IQR) years | 6.5(3-10) |
|---|---|
| Sex | |
| Male [n(%)] | 23(67.6) |
| Female [n(%)] | 11(31.4) |
| Day of illness at admission [median(IQR)] | 5(4-7) |
| Blood pressure | |
| SBP [median(IQR)] | 97(87.5-100) |
| DBP [median(IQR)] | 60(50-60) |
| Abnormal CVS findings [n(%)] | |
| Presence of Gallop/Murmur & Congestive hepatomegaly | 4(11.7%) |
| ECG abnormality (n=15) | 8(23.5%) |
| Sinus tachyacrdia, Sinus brady cardia & non specific T wave changes | |
| Shock | 7(20.6) |
| Total [n(%)] | 2(5.9) |
| Compensated [n(%)] | 5(14.7) |
| Hypotensive [n(%)] | |
| Parameters | Number (abnormal %) |
| NT-Pro BNP (n=27) | 22(64.7) |
| Troponin T (n=34) | 9(26.5) |
| CPK-MB (n=7) | 1(2.9) |
| D-dimer (n=30) | 28(82.4) |
IQR: Interquartile range, SBP: Systolic blood pressure, DBP: Diastolic blood pressure, CVS: Cardiovascular system, NT-ProBNP: N terminal Pro B type Natriuretic Peptide, CPK: Creatine phosphokinase
Among the laboratory markers, NT-Pro BNP, Troponin-T, CPK-total, CPK-MB, and D-dimer, D- dimer was elevated in 28 (82.4%) patients [Table 1].
Out of 34 MIS-C patients, 15 had ECG, and abnormalities were noted in eight children. The most common abnormality noted were sinus tachycardia, sinus bradycardia, and non-specific T wave changes. Since a majority of the children had predominantly echocardiographic abnormality than rhythm abnormality. So ECG was not done for all children recruited in this study.
Among the 34 patients, 27 (79.4%) had abnormal echocardiograms. The abnormalities noted were coronary abnormalities such as dilation and aneurysm, chamber dilatation, valvular regurgitation, decreased LV function, and pericardial effusion [Table 2].
| Parameters | Patient number (%) |
|---|---|
| Any abnormality | 27 (79.4) |
| Coronary abnormality | 12(35.2) |
| Dilatation | 5(14.7) |
| Aneurysm | 7(20.5) |
| Chamber dilatation | 1(2.9) |
| Valvular regurgitation | 11(32.4) |
| Abnormal LV function | 13(38.2) |
| Mild severe | 11(32.3) |
| 2(5.8) | |
| 0 | |
| Pericardial effusion | 19(70.3) |
| Coronary dilatation | LMCA-1 ,LAD-4 |
| Coronary aneurysm | LMCA-4,LAD-5,RCA-2 |
LMCA: Left main coronary artery, LAD: Left anterior descending, RCA: Right coronary artery
Among the coronary abnormalities, isolated aneurysms were seen in 5 (14.7%) patients, and 7 (20.6%) patients had both dilation and aneurysm. Among 12 patients with coronary abnormalities, the left anterior descending artery (LAD) (9/12) was the most involved artery, followed by the left main coronary artery (LMCA) (5/12). The aneurysms were mostly small aneurysms; only one patient had a moderate aneurysm of LMCA [Table 2].
In our study, 55.8% need pediatric intensive care unit (PICU) care, with a median length of PICU stay was 2.8 days (1–4) and a median length of hospital stay is 5.9 days (5–7).
MIS-C patients were followed up at 2 weeks and 6 weeks after discharge; 26 (76.4%) patients had follow-up data, remaining eight patients had not turned up for follow-up. Among the 27 patients with abnormal echocardiograms, 20 (58.8%) patients had follow-up echocardiograms. Among the patients who had been followed up with echocardiogram, 8 (23.5%) patients had two follow-ups at 2 weeks and 6 weeks after discharge, 8 (23.5%) patients had only one follow-up at 2 weeks after discharge, and 7 (20.5%) patients had only one follow-up at 6 weeks after discharge.
Analyzing the follow-up echocardiogram at 2 weeks after discharge, only one patient had persistence of coronary aneurysm at 2 weeks, which resolved subsequently at 6 weeks follow-up. All other abnormalities noted at admission in all patients were resolved at 2 weeks follow-up. At 6 weeks follow-up after discharge, all had normal echocardiograms and their previous abnormalities were resolved completely.
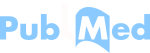
Scatter plot diagram of Z-score values of coronary arteries at admission were noted [Figure 1]. A Z-score of above 2 is abnormal, as is seen in Figure 1; a significant number of patients had abnormal Z-score at admission; however, only one had persistence of coronary abnormality at 2 weeks, and all Z-scores were normal at 6 weeks. Among the 34 patients, only 6 (17.6%) patients had repeat cardiac biochemical markers, and all six patients had normal values during follow-up at 2 weeks. As most of the children at the time of discharge, their biomarkers levels came back to normal, and only children with high levels were repeated during follow-up. The eight patients who have been missing during follow-up were contacted through telephone and their clinical well-being was confirmed.
- Z-scores of coronary arteries at admission. LMCA: Left main coronary artery, LAD: Left anterior descending, LCX: Left circumflex artery, RCA: Right coronary artery.
The patients received various treatments, including intravenous immunoglobulin (IVIG), steroids, aspirin, and different cardiac drugs. IVIG was given at a dose of 2 g/kg for children presented with cardiac manifestations alone (18/34). Steroids doses were given as a pulse dose of about 30 mg/kg in 7 (20.6%) patients and as 2 mg/kg in 22 (64.7%) patients. Although oxygen requirement was present in some (20.5%) patients, none of them were mechanically ventilated.
Summary
The median age of the population is 6.5 years with IQR 3–10
Among the inflammatory markers, CRP and D-dimer were markedly elevated
55.8% need PICU care, with a median length of PICU stay was 2.8 days (1–4) and a median length of hospital stay is 5.9 days (5–7)
Eight participants had abnormal ECG. The most common abnormality noted were sinus tachycardia/sinus bradycardia and non-specific T wave changes.
Twenty-seven had an abnormal echocardiogram, of which 12 had coronary abnormality. Seven children had dilatation with aneurysm, and five children had isolated aneurysm. LAD is the most common artery involved, followed by LMCA
A total (n = 34) 18 received IVIG, and seven participants had pulse dose steroids (30 mg/kg)
Twenty-two had standard 2 mg/kg.
Oxygen requirement were present in 20.5% of patients; none of them were mechanically ventilated, with nil mortality.
DISCUSSION
There are limited studies focusing solely on the cardiac manifestations along with the follow-up data in MIS-C, especially in India. Our study has evaluated the cardiac manifestations due to MIS-C by echocardiogram and the outcome and follow-up changes at 2 weeks, 6 weeks, and till the end of the study period. All the MIS-C patients included in the study were previously healthy children. The median age of our population was 6.5 years. Similar to this, other studies[18,19] have also demonstrated that MIS-C patients are usually older compared to classical Kawasaki disease, as described in various reports.[20] In the present study, the median day of illness of patients at admission was 5 days. The median pulse rate was 118 beats/min, and systolic and diastolic blood pressure was 97 mmHg and 60 mmHg, respectively. These values are similar to those reported by Matsubara et al., where the median pulse rate was 116 beats/min, and systolic and diastolic blood pressure were 99 mmHg and 56 mmHg, respectively.[20]
Clinically, cardiac manifestations were assessed with abnormal cardiovascular findings, congestive hepatomegaly, and the presence of shock. Abnormal cardiovascular findings were present in 11.7%, and congestive hepatomegaly was present in 11.8%. In our study, we have used CDC guidelines to diagnose MIS-C; we have reported 7 (20.6%) patients who presented with shock requiring fluid resuscitation and inotropes to recover. However, the incidence of cardiogenic and vasoplegic shock was observed in 40–80%of MIS-C cases in the literature. Campanello et al.,[14] in their study, found that all patients presented with cardiovascular manifestations and among the patients who presented with shock, none required inotropic support. We had only 15 patients with ECG data; among them, 8 (23.5%) had abnormal findings. Commonly noticed abnormalities were nonspecific T wave inversion, sinus tachycardia, sinus bradycardia, and QT prolongation. Regan et al., in their study, reported 67% of children with ECG abnormalities, and the most frequent findings were low QRS amplitude and transient T- wave inversion.[21] In our study, 27 (79.4%) patients with MIS-C had echocardiographic abnormalities; this is similar to reports of 75% of patients with echocardiographic abnormalities among MIS-C patients in a study by Kelly et al.;[22] In their study, the most common echocardiographic abnormality was reduced LVEF, noted in 58% patients. However, in our study, we have reported abnormal LV function in 13 (38.2%) patients with MIS-C.
Large case series in the literature have reported coronary artery abnormalities in approximately 13–26% of MIS-C patients.[23] In our study, using z-scores of 2–2.5 as dilation and ≥2.5 as an aneurysm, we have found 12 (35.2%) patients of MIS- C with coronary artery abnormalities. In our study, 26 (76.4%) patients had follow-up. We have follow-up at 2 weeks and 6 weeks after discharge. Analyzing the follow-up, only one child had a persistence coronary aneurysm at 2 weeks that too resolved at 6 weeks. All other abnormalities in other children had been resolved.
Among the laboratory markers, D- dimer was elevated in 28 (82.4%) patients. Similarly, a study by Dufort et al. reported elevated D-dimer in 91% of patients. However, the same study reported elevated troponin in 71% of patients, in contrast to our study, where we found troponin elevation in only 9 (26.5%) patients.[24]
The treatment of MIS-C has evolved over time. Children presenting with only fever, rash, and systemic inflammation without any signs of other organ damage require only close monitoring in an outpatient setting. However, close clinical follow-up must be ensured.[25] In the present study, oxygen requirement was present in 7 (20.5%) patients, but none were mechanically ventilated. However, Dhanalakshmi et al.[10] found a significant number of children (57%) developed hypotension, requiring admission to the PICU for vasoactive medications. Angurana et al. showed that most cases (85%) required PICU admission where they received nasal prong oxygen (40%), noninvasive (22.5%) and invasive (22.5%) ventilation, and vasoactive drug support (72.5%).[26].In our study, 55.8% of patients required admission to the PICU; in a similar study conducted in the United States in 2020, the majority of the patients (63.9%) had to be admitted to the intensive care unit (ICU).[27] In the present study, the various drugs given to our patients were immunoglobulin (52.9%) and steroids (64.7%). IVIG and glucocorticoids are considered the line agents for the treatment of MIS-C.[28] Both these therapies are the most frequently used immunomodulatory medications in MIS-C patients reported to date.[28,29] Evidence suggests that early initiation of IVIG and glucocorticoids in patients may potentially reduce ICU admissions and length of hospital stay.
The strength of this study is patient selection criteria as per CDC guidelines, and cardiac dysfunction not considered as mandatory criteria for MIS-C diagnosis. This could probably eliminate selection bias and our study had the opportunity to include patient spectrum from mild disease to severe disease. Moreover, echocardiography was performed by a single cardiologist to avoid observer bias. However, one limitation of this study was that children only under the age of 18 years were included; this might have resulted in the exclusion of MIS-C patients older than 18 years of age. Furthermore, it was a single-center study with medium sample size and follow-up data of few patients are lacking.
CONCLUSION
Cardiac manifestations in MIS-C are one of the most crucial and common systems to be involved which determines the severity and the prognosis in MIS-C patients. Our study suggests that prompt anti-inflammatory and multitarget therapy can potentially result in a favorable outcome, preventing further complications. However, further studies with larger sample sizes and longer follow-up periods are necessary to evaluate the long-term outcome for MIS-C patients.
Acknowledgments
I am grateful to Dr. Suvetha Kanappan, Professor of Community medicine, for helping me with the statistical analysis of this study.
Author contributions
Dr. Meenu Preethi was associated with the selection and recruitment of patients, data collection and monitoring. Dr. Muruganantham Balagurunathan conducted the examination of patients on follow-up and interpretation of data. Dr. Venkateshwaran Palanisamy and Dr. Jayavardhana Arumugam carried out the statistical analysis and interpretation, and Dr. Vinoth Doraisamy drafted the final report.
Ethical approval
The study was conducted after obtaining approval from the Institutional Human Ethics Committee (IHEC; Registration No. PSG/IHEC/2020/Appr/Exp/281) dated December 18, 2020.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript, and no images were manipulated using AI.
Financial support and sponsorship
Nil.
References
- Features, Evaluation, and Treatment of Coronavirus (COVID-19) In: StatPearls. Treasure Island, FL: StatPearls Publishing; 2023. Available from: https://www.ncbi.nlm.nih.gov/books/NBK554776 [Last accessed on 2023 Aug 18]
- [Google Scholar]
- COVID-19: A Review on the Novel Coronavirus Disease Evolution, Transmission, Detection, Control and Prevention. Viruses. 2021;13:202.
- [CrossRef] [PubMed] [Google Scholar]
- Clinical Characteristics of 140 Patients Infected with SARSCoV-2 in Wuhan, China. Allergy. 2020;75:1730-41.
- [CrossRef] [PubMed] [Google Scholar]
- COVID-19 pandemic: From Origins to Outcomes. A Comprehensive Review of Viral Pathogenesis, Clinical Manifestations, Diagnostic Evaluation, and Management. Infez Med. 2021;29:20-36.
- [Google Scholar]
- SARS-CoV-2 Infection in Children. N Engl J Med. 2020;382:1663-5.
- [CrossRef] [PubMed] [Google Scholar]
- Epidemiology of COVID-19 among Children in China. Pediatrics. 2020;145:e20200702.
- [CrossRef] [PubMed] [Google Scholar]
- Hyperinflammatory Shock in Children During COVID-19 Pandemic. Lancet. 2020;395:1607-8.
- [CrossRef] [PubMed] [Google Scholar]
- An Outbreak of Severe Kawasaki-Like Disease at the Italian Epicentre of the SARS-CoV-2 Epidemic: An Observational Cohort Study. Lancet. 2020;395:1771-8.
- [CrossRef] [PubMed] [Google Scholar]
- Acute Heart Failure in Multisystem Inflammatory Syndrome in Children in the Context of Global SARS-CoV-2 Pandemic. Circulation. 2020;142:429-36.
- [CrossRef] [PubMed] [Google Scholar]
- Epidemiological and Clinical Profile of Pediatric Inflammatory Multisystem Syndrome-Temporally Associated with SARS-CoV-2 (PIMSTS) in Indian Children. Indian Pediatr. 2020;57:1010-14.
- [CrossRef] [PubMed] [Google Scholar]
- Multisystem Inflammatory Syndrome in Children and Adolescents Temporally Related to COVID-19. 2020. Available from: https://www.who.int/news-room/commentaries/detail/multisystem-inflammatorysyndrome-in-children-and-adolescents-with-covid-19 [Last accessed on 2023 Dec 18]
- [Google Scholar]
- Guidance: Paediatric Multisystem Inflammatory Syndrome Temporally Associated with COVID-19. 2020. Available from: https://www.rcpch.ac.uk/resources/guidancepaediatric-multisysteminflammatorysyndrome-temporally-associated-covid-19-pims-guidance [Last accessed on 2023 Dec 18]
- [Google Scholar]
- Multisystem Inflammatory Syndrome in Children: A Systematic Review. EClinicalMedicine. 2020;26:100527.
- [CrossRef] [PubMed] [Google Scholar]
- Cardiovascular Manifestations in Multisystem Inflammatory Syndrome in Children (MIS-C) Associated with COVID-19 According to Age. Children (Basel). 2022;9:583.
- [CrossRef] [PubMed] [Google Scholar]
- Information for Healthcare Providers about Multisystem Inflammatory Syndrome in Children (MIS-C) 2023. Available from: https://www.information/for/healthcare/providers/about/multisystem/inflammatory/syndrome/in/children(mis-c)|cdc [Last accessed on 2023 Dec 18]
- [Google Scholar]
- Diagnosis, Treatment, and Long-Term Management of Kawasaki Disease: A Scientific Statement for Health Professionals From the American Heart Association [Published Correction Appears in Circulation 2019;140:e181-4] Circulation. 2017;135:e927-99.
- [Google Scholar]
- Clinical Characteristics of 58 Children with a Pediatric Inflammatory Multisystem Syndrome Temporally Associated with SARS-CoV-2. JAMA. 2020;324:259-69.
- [CrossRef] [PubMed] [Google Scholar]
- Longitudinal Echocardiographic Assessment of Coronary Arteries and Left Ventricular Function following Multisystem Inflammatory Syndrome in Children. J Pediatr. 2021;228:290-3.e1.
- [CrossRef] [PubMed] [Google Scholar]
- Kawasaki Disease in a Pediatric Intensive Care Unit: A Case-Control Study. Pediatrics. 2008;122:e786-90.
- [CrossRef] [PubMed] [Google Scholar]
- Echocardiographic Findings in Pediatric Multisystem Inflammatory Syndrome Associated With COVID-19 in the United States. J Am Coll Cardiol. 2020;76:1947-61.
- [CrossRef] [PubMed] [Google Scholar]
- Electrocardiographic Changes in Children with Multisystem Inflammation Associated with COVID-19: Associated with Coronavirus Disease 2019. J Pediatr. 2021;234:27-32.e2.
- [CrossRef] [PubMed] [Google Scholar]
- Multisystem Inflammatory Syndrome in Children: Cardiac Biomarker Profiles and Echocardiographic Findings in the Acute and Recovery Phases. J Am Soc Echocardiogr. 2020;33:1288-90.
- [CrossRef] [PubMed] [Google Scholar]
- Characteristics and Outcomes of US Children and Adolescents with Multisystem Inflammatory Syndrome in Children (MIS-C) Compared with Severe Acute COVID-19. JAMA. 2021;325:1074-87.
- [CrossRef] [PubMed] [Google Scholar]
- Multisystem Inflammatory Syndrome in Children in New York State. N Engl J Med. 2020;383:347-58.
- [CrossRef] [PubMed] [Google Scholar]
- Multisystem Inflammatory Syndrome in Children (MIS-C) During SARS-CoV-2 Pandemic in Brazil: A Multicenter, Prospective Cohort Study. J Pediatr (Rio J). 2021;97:354-61.
- [CrossRef] [PubMed] [Google Scholar]
- Intensive Care Needs and Short-Term Outcome of Multisystem Inflammatory Syndrome in Children (MIS-C): Experience from North India. J Trop Pediatr. 2021;67:fmab055.
- [CrossRef] [PubMed] [Google Scholar]
- Kawasaki-Like Multisystem Inflammatory Syndrome in Children During the Covid-19 Pandemic in Paris, France: Prospective Observational Study. BMJ. 2020;369:m2094.
- [CrossRef] [PubMed] [Google Scholar]
- Multisystem Inflammatory Syndrome Related to COVID-19 in Previously Healthy Children and Adolescents in New York City. JAMA. 2020;324:294-6.
- [CrossRef] [PubMed] [Google Scholar]
- Multisystem Inflammatory Syndrome in Children During the Coronavirus 2019 Pandemic: A Case Series. J Pediatric Infect Dis Soc. 2020;9:393-8.
- [CrossRef] [PubMed] [Google Scholar]




